Join the fun at Hanwell Carnival this Saturday & read our latest news – ESON Newsletter 12/06/19
")
|
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
")
‘GP at Hand’ with 51,596 Patients Threatens to Destabilise NHS Services in London
GP at Hand, Babylon Health’s virtual GP practice, has in just 18 months signed up and retained 51,596 patients. However, the ‘GPonline’ web site tells us that between November 2017 and March 2019 one in four of its patients had subsequently left the GP at Hand practice. 85% of those who signed up were aged between 20 and 39, and just over half of them were aged between 20 and 29.
GP at Hand is a Smartphone based app which facilitates online GP consultations at short notice. When you sign up to the virtual service, your registration at your place-based GP practice is cancelled. GP at Hand’s clinics include two in Fulham, a BUPA Health Clinic in Kings Cross, Lyca Health in Canary Wharf (part of the Lyca mobile phone operation), and one, the South Westminster Centre for Health, in Vincent Square. The latter appears to be run by diagnostic imaging specialists InHealth whose Cardiology Unit appears to have a link with Chelsea and Westminster Hospital.
In what the ‘Pulse’ web site describes as ‘destabilising’, it seems GP at Hand is in the process of registering its own NHS Primary Care Network (PCN). The aim of PCNs is collaborative working between GP practices, community, mental health, social care, pharmacy, hospital and voluntary services. Seven such PCNs have just been set up in Ealing. Each PCN can service up to 50,000 registered patients. GP leaders have expressed concerns that this ‘digital-first’ service will break the rule that PCN’s must exist within local boundaries. They predict that if virtual GP practices can become PCNs then it would destabilise all current NHS services in London.
We still await the results of the evaluation of GP at Hand carried out by Ipsos Mori which was first promised in March 2019. Publication of the results has been delayed three times now. NHS England and Hammersmith & Fulham (H&F) CCG commissioned this research which cost £250,000. The results were scheduled to be announced at the H&F CCG meeting on 21 May 2019. The presentation was cancelled at one hour’s notice, the CCG citing concerns about ‘factual accuracy’. Ipsos Mori, a 40 year old global leader in market research operating in 89 countries, is unlikely to be guilty of ‘factual inaccuracy’. However, ‘GPonline’ quotes Ipsos Mori researchers saying that ‘necessary datasets’ have not been made available to them.
Here we have a non-NHS provided service ‘approved’ by NHSE and personally endorsed by the Secretary of State for Health and Social Care. Maybe there are other virtual GP surgery offerings – maybe not. Apparently competitors include ‘Livi’ and ‘Push Doctor’. Have they (and possibly others) been ‘approved’ by NHSE? Perhaps GP at Hand should be nationalised and all GP surgeries mandated to offer it to all their patients. This would create a level playing field. Currently we have a tilted playing field which does not favour place-based GP surgeries in Hammersmith & London and elsewhere who are losing patients to GP at Hand.
GP at Hand appears to have a virtual monopoly in the virtual GP Surgery market. Although it is not illegal in England to set up a monopoly it is illegal to maintain one. Does Matt Hancock MP realise that by his publicly endorsing GP at Hand he is enabling the maintenance of a monopoly?
H&F CCG are facing an annual deficit of £37 million, 21.6 million of which stems from funding the growing patient lists of Fulham-based Dr Jefferies’ GP at Hand practice.
On 2 June 2019 ’The Sunday Times’ revealed worrying data about Babylon Health retrieved from the professional networking service ’LinkedIn’. Although high staff turnover rates are not unusual at tech star-ups, the fact the 37% of Babylon staff stay for 6 months or less is a real concern.
And Now We Have Virtual A&E…..
On 24 May 2019 ‘The Guardian’ exclusively revealed that sick patients in Birmingham will soon be able to seek emergency treatment by using their Smartphone instead of going immediately to a hospital A&E unit. They will engage in a two minute online triage to check their symptoms. This is yet another example of ‘demand management’ at work (see story below). The plan is to persuade 30% of those currently attending a place-based A&E to use a virtual A&E instead.
Not surprisingly Matt Hancock’s favourite ‘digital-first’ technology company Babylon Health is involved. A modified version of GP at Hand will be adopted by the University Hospitals Birmingham NHS Trust. The technology will be used to reduce face-to-face consultations in the areas of outpatients, chronic disease management (diabetes and heart problems) and in triage for Non-Elective hospital admissions.
NHS Says Charging for Nurse Training Will Result in 68,500 Unfilled Nursing Vacancies by 2013/24
The ‘Interim NHS Staff Plan’ has just been leaked and it makes worrying reading. It alleges that following the Government’s decision to abolish training bursaries for nurses, applications for nurse and midwifery training fell by 31% from 2016 to 2018. Clearly these dire predictions about staff shortages must have an impact on implementing the NHS Long Term Plan
The NHS Chief Executive Argues Against Policies He Has Championed
Simon Stevens has recently spoken in public about preventing the ‘hollowing out’ of District General Hospitals (DGHs). This is from the man who had allowed NHS North West London to hollow out Central Middlesex, Hammersmith and Ealing DGHs. The former two had their A&Es closed down in September 2014, and Ealing Hospital has in recent years been stripped of Maternity, Paediatrics, children’s A&E and Urology.
Delivering a lecture at the Royal Society of Medicine (RCM) in May 2019, Mr Stevens suggested that the NHS rethinks the DGH model to counter the risk of the health service deserting the ‘at risk communities’ many of them serve. This is all a bit rich when one considers that the hollowed-out Ealing Hospital is located in Southall, one of the most deprived areas in England.
Is what he is saying that he got it wrong in the past and he’ll put it right in the years to come? Well there’s nothing on in the ten year ‘NHS long Term Plan’ (LTP) published in January 2019 about reversing the hollowing out of DGHs.
So….how do we resolve these conflicting NHSE statements in the LTP and in the RCM lecture?
Is the Incidence of ‘Demand Management’ Initiatives a Potent Symbol of Neo-Liberal Dogma Permeating the NHS?
The concept of ‘demand management’ has a lot to do with ‘market’ situations when supply is dwindling – by design, by incompetence or by accident. Demand management initiatives somehow attempt to divert, bamboozle or even ‘educate’ the demander, resulting in their demands not being met or supply being delayed. If chocolate bars become in short supply demand management could raise prices or it could point out that too much chocolate is bad for you and offer the demander fruit (in greater supply) instead.
In the NHS since at least 2010, reducing the number of District General Hospitals (DGHs) and the number of hospital beds has been a design mandate. Hospitals are expensive places to run and NHS bosses started downgrading DGHs and reducing bed numbers as a way to cut costs. In NHS North West London (NWL) in 2012 bosses accepted the wisdom of management consultants McKinsey & Co that 40% of patients in Acute beds should not be there. Reducing bed numbers by 40% was the plan, but this plan was finally abandoned in March 2019. However in the 28 May 2019 NHS NWL commissioning reform paper, we are told that 30% of patients in Acute beds should not be there.
Whether by design, incompetence or accident, the number of doctors and nurses at work in the NHS is inadequate. In April 2019 NHS Improvement announced there were 100,521 NHS staff vacancies in England.
Various demand management techniques have been tried to reduce the number of people attending and being admitted to hospital. These include:
+ efforts to treat patients at home or in doctors’ surgeries (instead of in hospital)
+ attempts to make people lead healthier lives
+ initiatives to detect and treat potentially serious illnesses in their early stages which reduces the need for patients to enter intensive care in hospital
+ telephone voice and Smartphone online triage and treatment – hoping this will deter patients from turning up at GP surgeries, hospital Urgent Care Centres and hospital A&E departments.
+ ‘referral facilitation’ – slowing down, changing, or rejecting GP patient referrals to see hospital consultants
Some of these techniques have proved successful and some have failed.
If you want to see your usual GP it’s not unusual these days to have to wait three weeks for the privilege. Two requests in recent years for over £70 million to expand some GP surgeries in North West London have fallen on deaf ears at NHS England and the Department of Health.
Government smoking bans have been successful in reducing self-harm through nicotine/tar ingestion. However campaigns aimed at reducing self-harm from many other forms of substance abuse have had little success.
Initiatives with the elderly in detecting early stage bowel cancer, encouraging them to have flu jabs and self-checking their blood pressure at home have no doubt enjoyed some success. However there have been few publicised successful initiatives in detecting and treating early onset mental illnesses in children of all ages.
The jury is still out as to whether virtual GP surgeries, e.g. GP at Hand, are safe and effective and whether they might prove to be a universal panacea in Primary, Community and Secondary Care demand management.
In Ealing a referral facilitation service has been operating for a few years. A second GP reviews your GP’s referral for you to see a consultant. Well, it’s just been decided to discontinue this service in Ealing as allegedly it was proving to be a waste of money.
In the current NHS Long Perm Plan (LTP) the new Primary Care Networks (PCNs) will be financially rewarded if there are reductions in Acute hospital admissions amongst their 30,000 to 50,000 registered patient populations.
Also in the LTP, PCNs are expected to form multi-discipline teams to visit and treat patients at home in attempts to reduce the number of patients attending and being admitted to DGHs. This multi-discipline team approach has been tried throughout NHS North West London in recent years. Anecdotally I hear that it has been largely abandoned as it proved difficult to organise.
Reducing ‘bed blocking’ has gained much press attention in recent years. But has much been achieved in reducing it? At Ealing Hospital bed blocking, often by mentally ill and elderly patients, has effectively reduced the available beds even more. Because the number of specialist mental health beds have been reduced it’s often very difficult to discharge seriously ill mental patients. Government cuts to Local Authority funding have often resulted in much reduced care home capacity and home care services, sometimes making it impossible for recovering elderly patients to be safely discharged from hospital.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
PLEASE SIGN OUR PETITION HERE
|
")
NHS Integrated Care Providers (ICPs) – Do They Exist? When Will They Exist?
The public consultation on the ICP contract ended on 26 October 2018. By now ICP contracts should have been signed in Dudley and in Greater Manchester. However I can find no news announcements or web site updates announcing such events. NHS England’s (NHSE’s) web site states that ‘….the ICP contract…in its updated form…available…from Spring 2019’. So – can we expect this within the next few weeks? Probably not as the NHS consistently misses its self-imposed deadlines.
For the confused, NHSE seems to use the terms ICP and ICS as and when it chooses. The two acronyms apparently are interchangeable.
Of course what happens every few years in the NHS these days is that its bosses throw all the balls up in the air. This latest ball throwing happened in January 2019, with publication of the NHS Long Term Plan (LTP). The ten year LTP replaces the October 2014 NHS Five Year View. The LTP states that ‘ICSs are central to the delivery of the LTP’; ‘By April 2021 ICSs will cover the whole country’; ‘A single CCG for each ICS area’. In February 2019 NHSE set out its desire to bring in new Government legislation to make it easy for new NHS Trusts to be set up to become ICS/ICPs. On the ground in NHS North West London (NWL), a new care commissioner will have to be created – the NWL Clinical Commissioning Group – to which the new contracted NWL ICS/ICP will be accountable.
The LTP also points the way towards a transformation in Primary Care. A separate NHSE/BMA January 2019 paper outlines these imminent changes. I review this paper later in this newsletter.
Another aspect of the LTP with regard to CCGs is the appointment of the Accountable Officer. The LTP states that NHSE will ‘designate the Council’s Chief Executive or Director of Adult Services as the CCG Accountable Officer’. This would eliminate the current NHS NWL Collaboration of CCGs Accountable Officer Mark Easton as a candidate in the new NWL CCG and open up the choice of eight Local Authority Chief Executives and eight Local Authority Adult Services Directors as candidates.
The LTP goes into ‘blue sky’ mode by predicting ‘….future proposals for social care and health integration in the forthcoming (Government) Green Paper on adult social care’. This paper was first promised for publication in summer, then ’before the end of 2018’ and now goodness knows when. However as social care is such a mess one might question the usefulness of the five Governmental Social Care Green Papers published since 1999.
NHS NWL’s 2012 ‘Shaping a Healthier Future’ (SaHF) Cancelled and NHS NWL’s 2016 Sustainability & Transformation Plan (STP) to be Abandoned – One Wonders What the Life Expectancy Will Be of the Yet To be Born NHS NWL ‘Long Term Plan’ (LTP)
At the latest meeting of the NHS North West London (NWL) Collaboration of the Eight Clinical Commissioning Groups (CCGs) on 2 May 2019 there was much line drawing under the SaHF and the STP. The new kid on the block in terms of a plan will be NHS NWL’s regional version of the NHS England (NHSE) LTP published in January 2019. However NHS NWL has been slow to even respond to the new national ten year LTP never mind engage with local stakeholders in formulating an NWL LTP. Healthwatch – allegedly the patients’ consumer watchdog – is being employed to collect feedback on the LTP. See www.healthwatch.co.uk/what-would-you-do.
Ground-breaking commitments were made at this meeting by NHS NWL bosses to active engagement with Ealing Save Our NHS (ESON) and Save Our Hospitals – Hammersmith (SOH) in formulating this regional LTP. However, the well publicised (but possibly not well advanced), plan by NHS NWL to select a 4,000 person standing panel to review ongoing care transformations is as yet not in place.
I’m very supportive of the KONP critique of the national LTP (see below) and I’m concerned that the NWL regional version will just ’parrot’ the national version. However of much more tangible significance was the announcement that in 2019/20 the NWL financial plan involves cutting its £3.6 billion annual costs by £100 million. If achieved, this will mean lots of ‘demand management’ initiatives to ration care.
Yet more turbulence is expected in NHS NWL this year as it wrestles with eliminating eight local CCGs and creating a new regional CCG. Sadly some quite well paid executives will fall off their lucrative CCG gravy trains. However only confusion appears to be the target of the body which might deliver the new CCG’s purchased services. The emerging regional Integrated Care Partnership/Integrated Care System (ICP/ICS) will attempt to bring together a host of care service suppliers – NHS Trusts, Local Authorities, private care companies, charities, voluntary groups. Attempts to achieve this ‘seamless’ co-operation have been hampered in the past by Local Authority opposition of SaHF and the STP, especially in Ealing and Hammersmith & Fulham.
As for apportioning blame for the £235 million spent on the now cancelled 2012 SaHF and the no doubt tens of £millions spent on the about to be abandoned 2016 STP, Accountable Officer Mark Easton said at the meeting that ’no-one was to blame’. I didn’t know whether to laugh or cry at that point in the meeting.
To discover that money is being spent on refurbishing NHS NWL headquarters offices in Marylebone Road, London seems massively inappropriate. This was the location of SaHF staff and not only that, there is a repair bill backlog of £729 million for just four of the NHS NWL Major Hospitals.
The Transformation of GP Services – The Story So Far
It’s now over six years since I began researching and reporting on changes to NHS healthcare services nationally, regionally and locally. During this period the term ‘transformation’ has gained popularity with NHS bosses to label these changes. How has transformation impacted GP services since 2013?
Waiting Times
No-one will dispute that waiting times to see a GP have got considerably longer since 2013. Lots of reasons have been suggested for this. These include an increase in demand from an ageing population having multiple medical conditions/ illnesses. On the supply side GP numbers have declined since 2015, and we have only marginally more GPs this year than last year.
Overworked GPs
A recent survey by ‘Pulse’ magazine/web site revealed that GPs are seeing up to 60 patients a day – double the number they consider safe.
A Post Code Lottery for Performance?
One way of profiling GP surgery performance is to research the number of annual Non-Elective (NEL) admissions to hospital per 1,000 Weighted Patients in each surgery, town or across the region. These NEL admissions are mostly Emergency admissions. Local researcher Tony Brewer has revealed that using the NHS’s own data there are more than double the number in Ealing (80.8) compared with Westminster (32.81). There are even wide variations across Ealing itself – with patients at surgeries in Acton (68.80) registering much lower NELs than across the rest of Ealing (from 73.15 –88.95)
GP Referrals to Consultants
In 2013 if your GP in Ealing referred you to a consultant, an appointment was made and you’d go to see the consultant. These days life is just not that simple. Every GP referral is intercepted by the Referral Facilitation Service (RFS). The RFS, run by a private contractor, will employ a GP to ‘second guess’ your GP. This intercepting GP could cancel the referral, change the referral or allow the referral. One can only presume that the RFS is all about reducing the number of GP referrals and cutting costs. In management consultancy jargon this approach to rationing a service supply is referred to as ‘demand management’.
Use of Technology
For those with mobile phones the texting service by GP surgeries has clearly helped with reminding patients about their appointments and expediting follow-ups to test results. Relatively inexpensive blood pressure monitors have been purchased by patients and this cuts down visits to surgeries just to have your blood pressure checked. However some technology use is proving disruptive and some question its efficacy. Babylon Technology’s ‘GP at Hand’ is the main culprit here.
GP at Hand
Introduced in London in 2017 this Smartphone-based virtual GP surgery has now more than 48,000 patients. Online consultations are available 24/7 at short notice. The original service was operated out of Dr Jefferies’ surgery in Fulham. numerous ‘place-based’ GP surgeries have lost patients and NHS funds to Dr Jefferies.
Concerns about the online service are varied. Pregnant women and mentally ill patients are seemingly not welcome as patients. Some question the effectiveness and safety of the service and others see it as a threat to place-based GP surgeries. NHS England and Hammersmith & Fulham (H&F) CCG invested £250,000 with Ipsos Mori in 2018 to carry out a full scale, year-long review of GP at Hand. The research report was promised by March 2019. No sign of it yet but NHS England has already agreed to an expansion of the service to Birmingham. H&F CCG has gone into considerable debt, largely as a result of having to pay-out £26.2million to Dr Jefferies for his new patients (many presumably out of Borough) in 2018 – 2020.
Clinical Commissioning Groups CCGs)
In recent years Ealing’s 76 GP surgeries have been commissioned by Ealing CCG. Given that the 2012 Health & Social Care Act created CCGs as GP-led it’s been astonishing that conflict of interest seemingly plays no part in Ealing GP-led CCG purchasing of Ealing GP services!
Ealing GP Federation (EGF)
This private company, in which all 76 Ealing GP surgeries are shareholders, did not exist in 2013. Founded in October 2014 this non-statutory body ‘…allows for greater collaboration between practices’. Its web site provides few clues as to why the federation actually exists.
The Transformation of GP Services – The Future Does Not Look Promising
In January 2019, NHSE and the BMA published ‘Investment and evolution: a Five-year framework for GP contract reform to implement the NHS Long Term Plan’. Some of the GPs who found time to read and digest this 108 page/50,000+ word document have expressed their dismay about its content. If the framework is implemented, they say, it will lead to a deteriorating and rationed GP service and move us closer to adopting a US style privatised healthcare system. However, some GPs welcome any attempts to enable GP co-operation and believe change is desperately needed.
An extra £4.5 billion is apparently to be invested in community-based care (however that is defined) by 2023/24. At the heart of the new ‘framework’ is yet another new GP contract – The Primary Care Network Contract (PCNC). There is a guaranteed additional payment of £1:76 per patient if /when GPs sign their PCNC. Each GP must sign this contract by 30 June 2019 (it was originally 15 May 2019 – but this is normal NHSE re-scheduling….). Activation was scheduled for July 2019 – no doubt this will get re-scheduled also. This contract promises GPs more money – but at what ‘cost’?
GP practice patient lists must be handed over to the GP’s Primary Care Network (PCN). Each PCN will comprise 30,000 to 50,000 patients. The PCNs report to the regional Integrated Care System (ICS) and the lists will be available to the ICS. Each PCN will have an Accountable Clinical Director. How the PCN in Ealing will relate to the Ealing GP Federation is somewhat unclear.
GPs will have to take on new tasks. These include structured medication reviews, Care Home visits, anticipatory care, personalised care, supporting early cancer diagnosis, cardio-vascular disease prevention and diagnosis, and tackling inequalities. GP appraisals and revalidations will take up valuable GP time. GP performance and activities will be monitored to ensure that GPs are adhering to ‘corporate policy’. Detailed electronic patient records will have to be kept and electronic dashboards will monitor everything and will form the basis for evaluating what GPs get paid.
GPs will be financially incentivised to reduce the number of patients admitted to Acute hospitals. They will also be part of multi-disciplinary teams which will visit sick patients at home in order to prevent Acute hospital admissions. GPs will not lead these teams and the teams will follow protocols and pathways. There are obvious conflicts of interest issues here for GPs if they feel their patient should be hospitalised and the system ‘says no’. There will be sharing of cost savings but the savings will not go to the GPs they will go to the PCN.
More staff will be hired, trained and paid for, but these will mostly not be GPs. 20,000 additional staff are promised by 2023/24. They will include pharmacists, paramedics, physiotherapists, mental health therapists, associate physicians, social care prescribing link workers, and specialist receptionists. In this way Primary Care in England will become de-professionalised. There is a recommitment to the historic NHSE promise to recruit 5,000 more GPs but an acceptance that this amounted to only a ’marginal’ increase in 2017/18.
All patients will, apparently, have digital access to their full medical records from 2020. It’s interesting to point out here that £11 billion was wasted in failing to implement online medical records access from 2002 to 2013 – and now it’s being offered next year!
Virtual GP practices are to be encouraged and expanded. By 2021 every patient will be able to join a virtual GP practice and have online consultations with a GP. In view of the chaos and disruption cause by 48,000 GP at Hand patients in West London, who knows what chaos and disruption to place-based GP practices will occur when we have say five million virtual GP practice patients throughout England? With the massive elimination of face-to-face patient consultation with the same doctor, continuity of care comes to an end. Online consultations are unlikely to ever take place with the same GP.
Just how much does the general public, the press, NHS staff and GPs themselves know about these transformation plans and their implications? If GPs don’t sign up to the new contract, how will they be ‘punished’ one wonders?
KONP Advocates Scrapping Section 75 in the 2012 Health & Social Care Act; Discontinuing Any Form of Competitive Tendering; and an End to the Market System in the NHS
In its submission to NHS England (NHSE) – responding to the NHS Long Term Plan and draft primary legislation public consultation – Keep Our NHS Public (KONP) wants an end to Section 75. Section 75 enforces compulsory tendering. In fact KONP wants an end to any form of competitive tendering and the dropping of the market system which separates purchasers from service suppliers. KONP points out that whilst it agrees with the proposal to remove the Competition and Markets Authorities role, it disagrees with NHSE seeking powers to force through mergers. Mergers have led to centralisation, cost cutting and remote decision making.
KONP is also opposed to the ‘Payment by Results’ system. It sees this as breaking up block contracts and service level agreements – leading to NHS services being outsourced to private providers. Integrated Care Provision in the form of new NHS trusts ‘…to deliver integrated care’ is seen by KONP as more of the disintegrated services that we have now. Finally, KONP wants the repeal of the 2012 Act and advancement of the NHS Reinstatement Bill.
KONP was founded in 2005. See http://keepournhspublic.com for more.
| Judging by the continuous stream of messages that we have received over the last few weeks, there is no doubt about the delight felt by people across the Borough that Ealing Hospital is to remain as a proper acute hospital. A very popular theme in many messages was that ‘we stood together as a united community’. A bit of People Power goes a long way – something that the Government and NHS bosses never understood. They thought we would all give up eventually, but they were so wrong! |
| After 7 years of hard work by so many people it’s fantastic to be able to celebrate, so Ealing Save Our NHS is having a celebration. We are therefore inviting those of you who helped in any way to achieve this great success for our community, to join us. There will also be hospital staff and local politicians, all raising a glass together! |
| Get in touch for more information! |
| Our planned Street Stall this Saturday in Ealing Broadway, 11.00 – 1.00pmnear M&S has a very different message then usual! |
| Instead of ‘Save Ealing Hospital, Dump SaHF ‘, our latest leaflet (here) now reads: |
| Of course, NHS bosses have refused to admit they have retreated, or for that matter offered any apology for the scandalous waste of money (at least £72 Million). Nor have they apologised for the closure of maternity & acute children’s services or the demoralisation of staff at Ealing Hospital. We certainly won’t be letting them off the hook, and intend to fight on to stop the threat of future cuts and restore our lost vital services. |
| If you can help give out leaflets on Saturday that would be great. It will be lovely to give people some good news at last. |
| Ealing Save Our NHS and our sister campaign, Save Our Hospitals (Hammersmith & Charing X) are featured on the front page of the national ‘Health Campaigns Together’ newspaper. We are both part of a family of campaigns up and down the country and together we have kept up the pressure on health bosses and the Government against cuts to hospitals and privatisation. |
| You can read the story and more here |
| This was planned before the announcement that the Shaping a Healthier Future plans were finally dead. So the focus of our meeting will be a bit different then our usual ‘Save Ealing Hospital’. We will certainly have a speaker on the Government’s NHS Long Term Plan and its impact on our local NHS, including GP services, and want to discuss where next for Ealing Hospital, now the axe has been lifted. – please watch this space for updates |
| Ealing Save Our NHS has had a lively and imaginative contingent on the Carnival Procession for the last few years and this year we plan to participate again. Unlike previous years we may be more in Carnival spirit as we have much to celebrate. No doubt our much photographed bed will still make an appearance. |
Issue 77
8 April 2019
‘Transformation’ Special Issue
The cancellation of the NHS North West London (NWL) ‘Shaping a Healthier Future’ (SaHF) plan on 26 March 2019 was an event of local, regional and national significance.
The central tenet of SaHF – the reduction in the number of Acute/Major hospitals – has been with us as a ‘transformation’ shibboleth for a number of years. A paper by American management consultant gurus McKinsey & Co published in 2009 famously alleged that 40% of all patients in Acute Hospital beds should not be there. (It’s hard to find any empirical evidence which supports what has become a ’Tablet of Stone’). McKinseys repeated this dogma at a World Economic Forum (WEF) meeting in Davos in April 2012. Attendees at that WEF meeting included the current Chief Executive, ex-Medical Director and the Strategy Director of NHS England (NHSE), two ex-Secretaries of State for Health, Liz Kendall MP, the bosses of BMI Health and the Nuffield Trust and the NHS property disposal expert, Robert Naylor.
A Failed Acute Reconfiguration Transformation
SaHF, announced in summer 2012, embodied the McKinsey metric and proposed closing 37% of the Acute hospital capacity in NWL in ‘at least three years’. On the ground that amounted to downgrading four of the nine Acute /’Major’ hospitals and transforming them into ‘Local’ hospitals with no A&E, no Intensive Care Unit, and no operating theatres. SaHF promised NWL’s 2.1 million residents ‘…changes that will improve care both in hospitals and the community…’. Also promised was ‘world -class healthcare outside of hospital’ in GP surgeries and in health centres. ‘Networks of GP practices will work with other providers of health and social care services to deliver co-ordinated healthcare to the local community.’ Cost savings of 4% would be achieved annually.
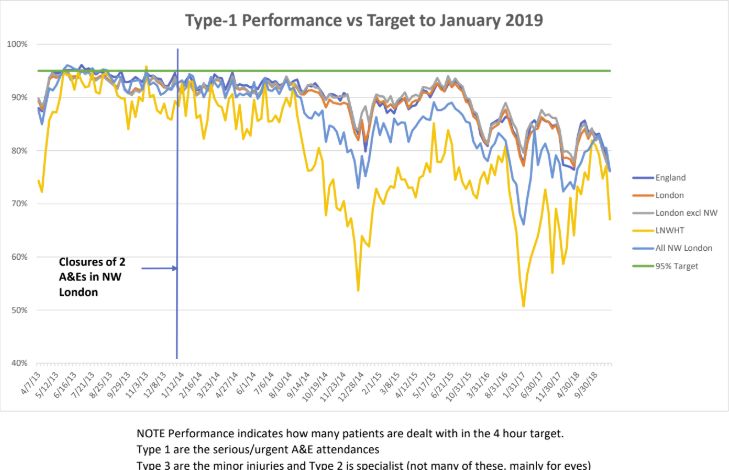
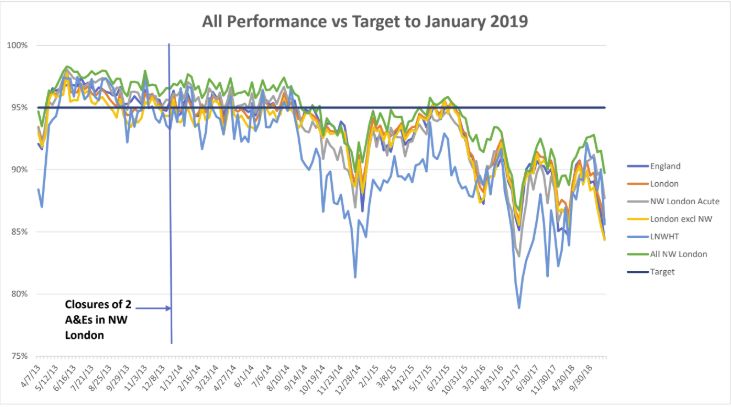
In September 2014 the SaHF closure of the A&E units at two NHS NWL Acute/Major hospitals decimated A&E performance throughout NWL to quickly become the worst in England. The two further A&E unit closures planned were delayed/abandoned and to this day the regional A&E performance has still not recovered. However the SaHF threat of downgrading Charing Cross and Ealing District General Hospitals has hung over the staff at these hospitals like the Sword of Damocles for almost seven years. Yet more grief was to be visited on Ealing Hospital in 2015 when Maternity was closed and in 2016 when Paediatrics was closed.
Inadequate SaHF Business Case
NHS NWL SaHF bosses ploughed ahead and in 2016 revealed more details of their business case. The SaHF ImBC Strategic Outline Case (SOC) for Acute reconfiguration 1 and 2 emerged. SOC1 covered building works required in ‘outer’ NWL hospitals, GP surgeries, and new Primary Care/out of hospital Hubs. £513 million was the breathtaking capital request. SOC2 covered building work in ‘inner‘ NWL and was estimated at £314 million. SOC1 was refused by NHS Improvement (NHSI) and NHSE London in September 2017. A second attempt at SOC1 occurred in July 2018 with a more modest capital request of £260 million. This was refused by implication in 2018 and finally went down in flames on 26 March 2019. The SOC2 capital request was never formalised and it was quietly buried by SaHF bosses in 2018.
Apart from Austerity and Brexit, what really killed the SaHF was its Acute reconfiguration business case proposition that Non Elective Admissions (NELs) – largely Emergency admissions – could be reduced significantly over time (probably by the McKinsey magical 40%). SaHF completely failed to convince NHSI and NHSE London financial bosses that it was making any progress at all to meet its own imposed annual NELs reduction target of 99,000 by 2025/26. Since 2013 no amount of increased GP or community services, specific new treatments or attempts to make more efficient use of hospital beds has had any impact on the annual level of NELs in NWL. In fact the total annual of NELs in 2017/18 were 181,632 and in 2013/14 they were 167,222. ‘Bed blocking’ didn’t help either. Elderly patients can’t be discharged if no places are available in care/nursing homes or family support is not available at home. Another major category is mentally ill patients. If no specialist mental health bed can be found then a patient can’t be discharged from an Acute hospital.
What Did SaHF Actually Cost?
Researcher Colin Standfield calculated in November 2017 that the management consultancy spend by NHS NWL since 2009/10 amounted to over £88 million. He recently re-calculated this and got it down to ‘just’ £72 million. Much, if not all, of this was SaHF related. There’s no easy way of calculating what the staff salary bill might have been for SaHF as it was a project and not a statutory NHS body.
Who Can be Held Responsible for the SaHF Failure?
Of the eight NHS NWL Clinical Commission Group (CCG) Chairs who signed their names to SaHF in 2012, four of them are still in post. They are Dr Mohini Parmar, Dr Tim Spicer, Dr Ian Goodman and Dr Nicola Burbidge. At least two of them are earning over £100,000/year. They must all consider their positions. The original SaHF Medical Director, Dr Mark Spencer moved into management consultancy a few years ago. However the current SaHF Medical Director, Susan La Brooy should also consider her position. The two NHS NWL Chief Officers behind the failed SaHF SOC1 £513 million bid (Clare Parker and Rob Larkman) gracefully resigned their posts in 2018. However the Accountable Officer responsible for the 2018 failed SaHF SOC1 £260 million bid, Mark Easton, is still in post and he surely must consider his position. Juliet Brown, Director of SaHF Implementation, must surely be made redundant.
What Can the Failed SaHF Tell us About Current and Future Transformations Like STPs and ICSs?
I find it hard to believe that all 44 NHS areas/’footprints’ were allowed to spend tens of £millions on management consultants to design’ prototype’ Acute reconfiguration projects. The 44 October 2016 Sustainability & Transformation Plans (STPs) throughout England borrow hugely from the SaHF approach (albeit with the addition of integrated healthcare and social care, and mental health). With SaHF failing, this calls into question the whole STP approach. Since 2017, STPs have morphed into Sustainability & Transformation Partnerships (again confusingly called STPs). In NWLthe STP was renamed the North West London Health and Care Partnership (HCP). The new NHS Long Term Plan has determined that all STPs will become Integrated Care Systems (ICSs) by April 2021.
NHS NWL STP Transformation To Be ‘Retired’?
Probably the primary goal of the NHS NWL STP/HCP is to plug the expected ‘do nothing’ annual funding gap of £1.41 billion by 2020/21. With just two years to go to meet this financial target who knows whether NHS NWL is on track to achieve this. Many commentators over the last two years have deduced that this financial STP target is unachievable and common sense tells me that they are right. I’m sure NHS NWL was disappointed to receive just £10 million funding in the 2018 round of national STP funding. There are plenty of SaHF ‘ghosts’ in the NHS NWL STP. One of them can be found in Delivery Area 5C. The downgrading of Ealing District General Hospital is cited here in the context of ‘…reducing demand for Acute services through investment in the proactive out of hospital care model enabled by investment in the Hubs’. We are back to Acute reconfiguration here and the need to radically reduce the number of NELs, which NHS NWL has failed miserably to do for over five years. Requests for capital funding to build Hubs were turned down in 2017 and in 2018.
It’s abundantly clear from recent comments in public by Mark Easton that the NHS Long Term Plan (LTP) presents NHS NWL with an opportunity to abandon its failing STP/HCP and carry out ‘re-modelling’ to produce an NHS NWL Integrated Care System (ICS). The fatal flaw in this, I suspect, is there is no compelling evidence that integrating healthcare and social care services will result in better care outcomes and reduced overall costs.
Will the NHS NWL ICS Transformation Go ‘Full Term’
However, what is clearly needed now is a STP/HCP rewrite to produce a deliverable ICS plan, aligned with the LTP. The architects of this new plan should not be authors of the SaHF or the STP/HCP or their management consultants. What is needed is new blood to create a viable plan based upon clear assumptions and credible evidence.
It would be painfully sad if this newsletter had to report in 2021 that the NHS NWL ICS was to be ‘re-modelled’ and replaced by a new acronym/plan. Surely at some point these repeated cycles of plan creation, failure, and re-branding have to come to an end and be replaced by stable, sustainable, adequately funded and maintained care services.
Finally what could tell us all a lot more about how and why SaHF failed is an independent Government inquiry or even an independent project review carried out by informed individuals who have had no involvement with SaHF. Surely by this means some valuable lessons could be learned from this expensive and, for some, painful failed attempt at transformation?
Eric Leach
| We are delighted to inform you that the Government has now withdrawn their support from the ‘Shaping a Healthier Future’ (SaHF) cuts plans. This means that Ealing & Charing Cross Hospitals are keeping their A&Es!! Along with the A&Es, wards will remain open and patients will be able to have treatment, operations and a bed at both hospitals. – Fantastic news and a great achievement for everyone who campaigned in both Boroughs. |
| None of this could have happened without the tremendous work done by campaigners, our local councils and everyone who helped by producing & giving out leaflets, running street stalls, signing petitions, attending protests, demonstrations, challenging the NHS bosses at meetings, doing the research and more. |
| The Government announcement on our hospitals: |
| On Tuesday 26th April, Matt Hancock (Secretary of State for Health & Social Care) made the following Statement in response to a question from the Conservative Chelsea & Fulham MP: |
| “Shaping a Healthier Future (SaHF) is no longer supported by the Dept for Health & Social Care, by NHS Improvement or by NHS England (national NHS bosses).The NHS will look at parts of the proposals that are in line with the Long Term Plan like the aspects of the plan that are focused on expanding the treatment of people in the community. But as for the changes in A&E in West London, for instance at Charing Cross Hospital that he mentions that are part of Shaping a Healthier Future, these will not happen”. |
| North West London NHS bosses accept Ealing & Charing Cross are here to stay! |
| Following the announcement in Parliament, NHS North West London issued a Statement, the key bit being – |
| “We will not be taking forward the plans as set out in SaHF for changes to Ealing and Charing Cross hospitals, but this does not mean that services across NW London will not change.” |
| You can read the full statement here – |
| Readers of our Newsletter will know that Ealing Save Our NHS thought that ‘Shaping a Healthier Future’ had been the ‘walking dead’ for some time. Despite all the money spent on community care and other ‘out of hospital’ services, North West London NHS has not been able to reduce demand for hospital beds – in fact demand is increasing! And, national NHS bosses had twice refused to fund North West London NHS’s bid for capital that would have allowed them to expand other A&Es and services to ‘replace’ Ealing Hospital. |
| There is no apology for the millions of pounds (at least £72 million) spent on management consultants to advise them on implementing SaHF, the upset caused to staff at our Hospital, and the closing of our Maternity, Childrens A&E & Charlie Chaplin Ward. In fact, quite the opposite, they claim that maternity care and emergency paediatric care have improved. It doesn’t seem that way to people in Ealing! |
| You can read Ealing Save Our NHS press release here – |
| And Ealing Council’s press release here – |
| What Next? |
| Ealing Save Our NHS will be discussing the next stage in our campaigning. As well as wasting millions of pounds of NHS money on a failed project, a huge amount of damage has been done to Ealing Hospital. We have lost services, staff and more. We will be demanding that our services are re-instated and that the Government funds the NHS. Please contact us if you would like to help. |
| In the meantime let’s enjoy our success. |

EALING SAVE OUR NHS PRESS RELEASE
Finally – at last, the Government has admitted the horrible ‘Shaping a Healthier Future Plan’ (SaHF) is not workable. It’s dead!
Former NHS England chief executive Sir David Nicholson had called these plans “the most significant reconfiguration project in the country”. But since they first announced the SaHF plans to cut nine major hospitals in North West London down to five, Ealing Save Our NHS has been campaigning against it side by side with many others including Save Our Hospitals Charing Cross and the Councils in Ealing and Hammersmith & Fulham.
SaHF had offices in posh Marylebone and spent tens of millions of pounds of NHS cash on management consultants. All for nothing.
 Now the Secretary of State for Health, Matt Hancock, has admitted that the Department of Health no longer supports it. The application for £500 million pounds by local health bosses had been turned down twice because the figures didn’t work.
Now the Secretary of State for Health, Matt Hancock, has admitted that the Department of Health no longer supports it. The application for £500 million pounds by local health bosses had been turned down twice because the figures didn’t work.
No surprise to us. They never worked.
A report from John Lister produced in 2012 for Ealing and Brent Trades Councils, clearly outlined that the whole thing was nonsense. So did subsequent reports commissioned by Ealing and Hammersmith & Fulham Councils.
Ealing Save Our NHS has distributed a quarter of a million leaflets on the streets, held protests, attended carnivals, organised parties, lobbies, petitions, car conveys and much else to spell out the truth, all paid for out of our own pockets and donations.
On the other side huge amounts of NHS money was spent on public relations staff and glossy leaflets to pretend that our health would mysteriously be improved if they closed departments, A&Es and hundreds of beds. It didn’t work.
Even then, after the funding was turned down and 7 years of a failed five year plan had gone by, local health bosses still carried on pretending the emperor was wearing clothes.
So what will happen now?
Ealing Save Our NHS will keep on campaigning. This disastrous SAHF plan has seen closure of two local A&Es, Central Middlesex and Hammersmith, as well as the closure of Ealing A&E to children. As a direct consequence, waiting times for Type 1 urgent A&E visits increased greatly. Ealing Hospital’s excellent maternity department was also closed, forcing Ealing mothers to travel and making continuity of care more difficult for many.
But health bosses appear to have learned nothing and to defend the indefensible. They try to conceal the A&E figures and deny there has been a problem. Mark Easton, the head of the North West London Clinical Commissioning Groups, in announcing the death of SaHF has just made the mind-boggling claim that maternity care and emergency paediatric care have improved. This is certainly not the view of local parents whose local services have closed!
Ealing Hospital remains seriously underfunded and in crisis. But at least there is a ray of sunshine – the horrible plan underlying all these cuts has gone and we can focus on calling for proper funding and restoration of local health services.
More information:
Oliver New 07931 198501
")
The NHS North West London ‘SHAPING A HEALTHIER FUTURE‘ TRANSFORMATION IS FINALLY ABANDONED By The Department of Health
Secretary of State Matt Hancock MP announced the end of SaHF in the House of Commons on 26 March 2019 in response to a question asked by Greg Hands MP for Chelsea and Fulham. This ends years of SaHF failings and NHS bosses being in complete denial. It also marks a campaigning victory for many people, especially Ealing Save Our NHS (ESON), Save Our Hospitals (Hammersmith & Fulham) and Brent Patient Voice.
Changes to Ealing and Charing Cross Hospitals mandated by SaHF will not now be implemented.
SaHF all started in 2012 with an awfully flawed public consultation which effectively set up nine NHS North West London ‘Major’ Acute hospitals to compete with each other for survival. SaHF promised ‘..changes that will improve care both in hospitals and the community and will save many lives each year’. Annual savings of 4% were promised. SaHF promised that these changes would take ‘at least three years.’ By 2013 Ealing Hospital and Charing Cross Hospitals were singled out in SaHF to be closed down as ‘Major’ hospitals. In September 2014 SaHF closed A&Es at both Central Middlesex and Hammersmith Hospitals. A&E performance throughout the whole of North West London dropped immediately and massively. It has never really recovered over the last 4.5 years. Subsequently Ealing Hospital ‘s Maternity unit and Paediatric units were closed down.
In 2015 Michael Mansfield QC led a masterful Independent Healthcare Commission which concluded that SaHF was neither affordable nor deliverable. In 2016 Hammersmith & Fulham and Ealing Council commissioned Roger Steer, John Lister and Sean Boyle to review SaHF and the related NHS NWL Sustainability and Transformation Plan (STP). The authors recommended that SaHF should be abolished/suspended.
In November 2017 after years of painstaking research and data collection Colin Standfield reported that NHS NWL had spent over £88 million on management consultancy since 2009/10 – the bulk of it on SaHF. What a tragic waste of public money.
No SaHF cost savings have been announced. In December 2016 SaHF asked NHS bosses for £513 million for building work, which was refused. NHSE/I London described the SaHF business case logic as ‘counterfactual’. In 2018 SaHF asked NHS bosses for £260 for building work. It received only £10 million but kept on believing it was going to get the big bucks – until today when reality hit hard.
A New Clinical Commissioning Group CCG) for NHS North West London (NWL) Could Mean 100s of Redundancies at the 8 NHS NWL CCGs
As a requirement of the January 2019 NHS Long Term Plan, an Integrated Care System (ICS) needs to be created for each CCG. At first I naively assumed this would mean eight ICSs in NHS NWL to ‘match’ the eight CCGs. But this is apparently not so. What seems to be on the cards is the creation of a new NHS NWL CCG which would commission the new NHS NWL ICS. As night follows day this new CCG would replace the existing eight CCGs.
This new ‘regional’ CCG would simply blow out of the water the original 2013 notion that CCGs would be locally led by local GPs who would have local knowledge. So how might a Southall GP sitting on the new NHS NWL CCG have any sort of knowledge of health care and social care issues in, say, Westminster?
I have not counted the staff in the eight NHS NWL CCGs, but as of 31 March 2019 there were 680 staff members in just four of the CCGs (Brent, Ealing, Hillingdon and Westminster CCGs). Surely the new CCG would not employ anything like this figure so one can assume lots of redundancies. Also no rational person would surely advocate that the 17 Public Relations staff currently employed by the eight CCGs would all be given jobs in the new NWL CCG.
It looks as if at a borough level in the absence of CCGs eight Integrated Care Partnerships (ICPs) will be established for each ‘town’. These ICPs would have no statutory legitimacy in terms of the 2012 Health and Social Care Act. The ICPs concept (originally conceived as ACPs) were STP vehicles for functional service delivery (not commissioning). In fact the 2016 NHS NWL STP cites ACPs to deliver elderly care in 2020/21. All very confusing.
The New Ealing Out Of Hospital (OOH) Services Single Supplier Initiative
On 14 February 2019 a 10 year Ealing OOH Services Single Supplier contract was signed by ‘West London and Ealing CCG’ (whatever body that might be) and West London NHS Trust (WLNT). WLNT is what used to be called West London Mental HealthTtrust and is the only NHS Trust which is based in Ealing.
The 2017 Ealing OOH Services single supplier proposals stated that the preferred provider would begin operation by the end of June 2019. A 1 May 2019 start date was also stated as a target. July 2019 is now the estimated start date being quoted by WLNT.
It will be interesting to discover when this service begins when the Single Point of Access (SPA) for Ealing OOH services will go live. In the 2017 plan, the SPA would go live (with clinical triage) by 1 October 2019. When the SPA does go live, it might well take a while for patients, service users and carers to understand to which healthcare and social care services the SPA relates. Of course it won’t deal directly with any OOH mental health services, but will refer callers to the mental health SPA.
Of the 15/16 members of the Strategic Oversight Partnership Board, who will ‘oversee’ the new Ealing OOH Services performance, four are Ealing Clinical Commissioning Group (ECCG) bosses. When the ECCG closes down by 2020/21 (and is replaced by a new North West London CCG) these four will have to be replaced.
Since 2017 Ealing Save Our NHS (ESON) has repeatedly asked ECCG to see a copy of the Ealing OOH Single Supplier business case. The ECCG is still refusing to supply this to ESON. Now that the contract has been awarded and the award presumably blessed by NHS England and the Department of Health bosses it seems ridiculous that ECCG should continue to withhold the business case.
|
|||||||||||||||||||||
|